Prescribing in the Larger Adult
Consider larger doses in the patients who weigh > 130 kg.
General Advice
- Body composition consists of fat mass (adipose tissue) and fat-free mass/lean bodyweight (protein including muscle, water and bone).
- Body Mass Index (BMI) is used to classify obesity but is unreliable for drug dosing (a person who is 150 cm 70 kg is obese but not large from a dosing perspective).
- Overweight patients have different proportions of fat mass and fat-free mass when compared to non-obese patients. See figure 1 below.
- Increases in fat-free mass correspond with an increase in drug clearance.
- Lipophilic drugs may have longer half-lives in people with more adipose tissue.
- For advice about specific medicines, discuss with the Ward Pharmacist or contact Medicines Information (
 80900).
80900).
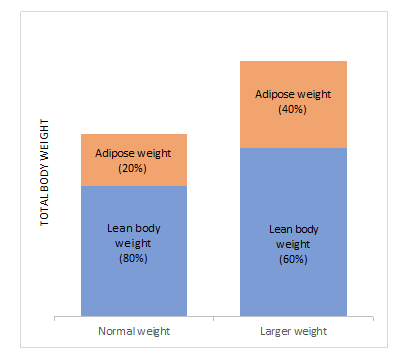
Figure 1: Proportion of fat mass and fat-free mass in normal weight and larger-weight patients.
Pharmacokinetic Considerations
Loading Doses
- Determined by the volume of distribution (Vd).
- Hydrophilic/water soluble drugs (such as beta-lactam antibiotics) have Vd that are not influenced by excess adipose tissue. However, larger patients typically have greater muscle mass, which does increase the Vd. Therefore, doses are slightly higher for this group compared to other patients.
- Lipophilic/fat soluble drugs (like phenytoin) disperse into adipose tissue readily which increases the Vd. Therefore, doses are higher in larger patients.
Maintenance Doses
- Determined by clearance.
- Lean weight – rather than total body weight – impacts maintenance dosing. Larger patients, regardless of whether they are overweight or not, have larger organ mass and blood flow. See figure 1 above.
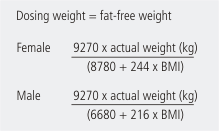
- Use this formula to calculate
 lean bodyweight/fat-free weight (dosing weight).
lean bodyweight/fat-free weight (dosing weight). - Normal dosing weights for a 170 cm tall, 70 kg person, are 44 kg for a female and 55 kg for a male. Heights only need to be accurate to within 10 cm.
- For metabolised drugs, the dose is estimated using this calculation.
Using renal function estimates
- One option is the Cockcroft and Gault equation.
- An alternative is the estimated glomerular filtration rate (eGFR) from the laboratory (mL/min/1.73 m2). However, this is inaccurate in patients > 130 kg without adjustment for Body Surface Area (BSA). For help with adjusting for BSA, contact the ward pharmacist.
Medicines of note when prescribing in larger adults
Beta lactam antibiotics (penicillins, cephalosporins etc.): larger doses should be used due to increased renal function. Use upper limit of normal dosing unless there is renal impairment.
Enoxaparin: Use actual bodyweight. Avoid 1.5 mg/kg every 24 hours in patients weighing over 100 kg as doses greater than 150 mg every 24 hours are expected to increase bleeding risk. If the calculated dose of enoxaparin using 1.5 mg/kg is greater than 150 mg every 24 hours, use 1 mg/kg and give it every 12 hours if creatinine clearance is at least 60 mL/min. We also recommend checking anti-Xa levels.
Aciclovir: Use ideal body weight for intravenous dosing.
Weight terms, definitions, and equations
Weight terms
|
Definition
|
Formula
|
Total body weight
(TBW)
|
Actual body weight of the person
|
Total kg
|
Ideal body weight
(IBW)
|
The optimal weight associated with maximum life expectancy for a given height
|
Male (kg) = 50 + [0.9 ×(Height (cm) − 152)]
Female (kg) = 45.5+ [0.9 × (Height(cm)–152)]
|
Adjusted body weight
|
Calculation adjustment for someone's actual body weight when they are overweight or obese
|
IBW (kg) + 0.4 (TBW (kg) – IBW (kg))
|
Lean body weight
|
Patient’s weight with adipose tissue removed
|
Formula as seen above
|

Topic Code: 93237